Accurate monitoring of haemophilia treatment
Preventive treatment of haemophilia has been around for over 60 years. Since then, there have been profound advancements in medicine and in recent years, the development of new drugs in haemophilia treatment has built and gained noticeable momentum of its own. Nevertheless, a challenge remains in ascertaining what needs to be taken into account during monitoring.
What needs to be considered during monitoring?
Available treatment options today are based on new recombinant products with an extended half-life (EHL factor concentrates). The products are achieved by modifying the coagulation factor, either by fusion of the Fc region of IgG1 or albumin, or by the addition of polyethylene glycol (PEG) in different molecular weights. Treatment strategies that do not involve factor replacement therapy are also becoming increasingly significant. Emicizumab, for instance, is a humanised bispecific monoclonal antibody for the treatment of haemophilia A (HA), which mimics the function of coagulation factor VIII. One-half of the antibody binds to activated coagulation factor IX (FIXa) and the other half to coagulation factor X (FX). The antibody can, thus, replace the activated factor VIII (FVIIIa), which is absent or barely present in HA patients.
Gene therapy
Another viable option for treating haemophilia patients is gene therapy. A complete functional copy of the coagulation factor gene, which is defective in haemophilia, is introduced into the patient’s body using genetically modified viruses (usually adeno-associated viruses, AAV). A targeted promoter controls the introduction of the gene into liver endothelial and sinusoid cells. Ideally, the patient’s body should be able to independently produce sufficient quantities of coagulation factor.
To avoid unwanted bleeding and long-term adverse effects reliable and accurate monitoring of treatment is extremely crucial for people with haemophilia.
Monitoring
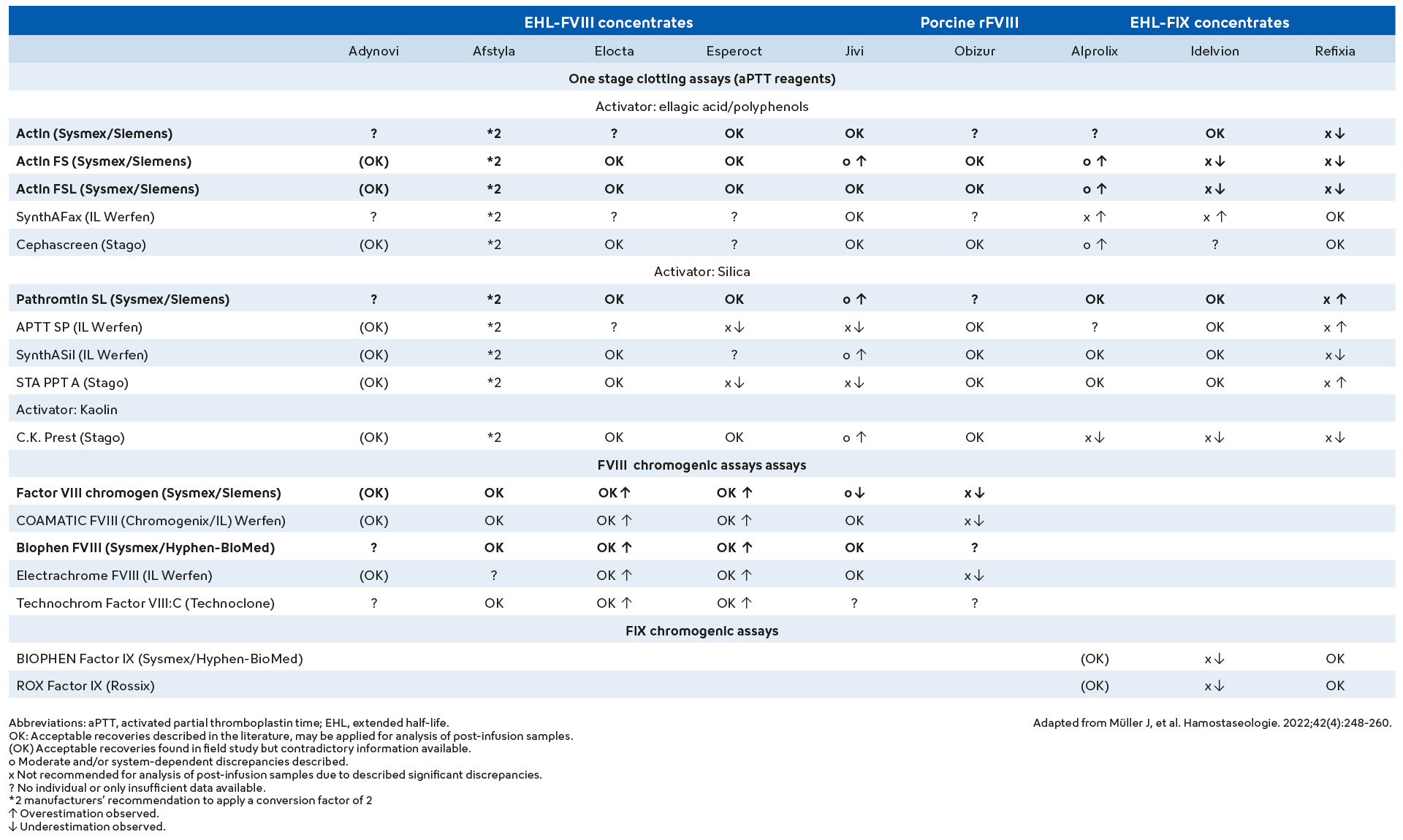
For the determination of FVIII and FIX levels, there are one-stage and two-stage coagulation assays as well as chromogenic assays (CSA). It is well known that the results of the various tests for hereditary haemophilia can differ - particularly in the mild forms. This also applies to monitoring treatment with human plasma-derived coagulation factor concentrates and full-length recombinant products. Nevertheless, one-stage coagulation and chromogenic assays generally allow for accurate and reliable treatment monitoring.
With the development of new recombinant EHL coagulation factors and so-called non-factor replacement therapies, new challenges have arisen for the laboratory. A dramatic over- or underestimation of factor activities may occur depending on the EHL product and the APTT reagent used. Although chromogenic assays are less sensitive to this phenomenon, the lab must ensure that the most suitable chromogenic assay is selected. For example, most silica-based APTT reagents should not be used to determine the infused FVIII concentration of Esperoct (N8 GP), because the FVIII concentration is underestimated during the use of this reagent. This is not the case for other non-silica-based APTT reagents. However, it should be noted that individual guidelines also exclude some non-silica-based APTT reagents from treatment monitoring with Esperoct.
For other recombinant products, the choice of assay method is not important as they can be measured correctly with both OSA and CSA. Comprehensive studies are now available and provide guidance for the selection of the most suitable one-stage or chromogenic assay for the EHL product used to treat the haemophilia patient.
Differences in the results of various one-stage APTT-based factor assays (OSA) can be attributed to several factors, such as the phospholipids used (whether of plant or animal origin or recombinant) and their concentration or the activator used. In addition, the choice of factor deficient plasma (e.g., the concentration of von Willebrand factor ‘VWF’ in factor VIII deficient plasma or only with residual activity) also critically impacts the determination of the factor concentration in patients with haemophilia. Other factors influencing the quality of haemophilia treatment monitoring include: the type of calibrator used — where assay-specific calibrators may be recommended in certain cases — the utilised analyser and test protocols, such as whether single or multiple dilution analyses are performed and the linearity of the test.
More often than not, the results obtained with OSAs tend to be higher than those obtained with CSAs and are most pronounced in patients with a mild form of haemophilia. However, the opposite may also occur; the result of a chromogenic assay corresponds to mild haemophilia, but the clinical picture relays a different story.
Which drug?
One-stage assays are not recommended for some EHL drugs since they underestimate factor activity. For some other drugs, this restriction only applies to the activator used for the APTT reagent.
Given the large number of different treatment approaches, it is crucial for the laboratory to know which drug the haemophilia patient is receiving to select the most suitable measurement method for treatment monitoring. For an overview of the assays that should, according to the manufacturer’s instructions as well as experts in the field, be used for monitoring the various treatment options for haemophilia, please refer to the table below.