
Scientific Calendar April 2020
Can XN-Series analysers automatically detect and resolve measurement interferences?
Yes, always
Yes, in certain cases
No
Congratulations!
That's the correct answer!
Sorry! That´s not completely correct!
Please try again
Sorry! That's not the correct answer!
Please try again
Notice
Please select at least one answer
Scientific background
Hyaluronic acid (HA), also called ‘hyaluronan’, is a component of the extracellular matrix distributed widely throughout connective, epithelial and neural tissues. Chemically, it is an anionic, non-sulfated glycosaminoglycan which forms high molecular weight polymers. Physiologically, HA contributes significantly to cell proliferation and migration and fulfils various functions in different tissues, e.g. a lubricating role in muscular connective tissues, involvement in tissue repair of skin or a lubricating component in synovial fluid. Quite a few mechanisms have been proposed for the involvement of HA in tumour malignancy. The concentration of HA is elevated in several inflammatory diseases and various carcinomas, including bladder, prostate, breast, lung and colon [1]. It has been closely correlated with tumour cell growth, proliferation, metastasis and angiogenesis. Studies have shown that highly metastatic tumour cells produce higher levels of HA than low metastatic counterparts [2].
Hyaluronidase is an enzyme that catalyses the degradation of hyaluronic acid by lowering its viscosity, which leads to increased membrane tissue permeability. Levels of hyaluronidase are elevated in many cancers [1]. Hyaluronidases are a family of five human enzymes namely hyaluronidase 1 - 4 and PH20. Three of these have measurable activity for endolytic HA hydrolysis; one acts primarily on chondroitin sulfate, and activity of the fifth has not yet been completely determined, but it is inactive toward HA.
Hyaluronidase-1 (Hyal1) is the major tumour-derived hyaluronidase. Clinically, Hyal1 expression can be used as a diagnostic marker to screen benign tissue and predict subsequent invasive breast cancer progression [3]. Hyal1 overexpression in breast cancer enhances motility and anchorage independent growth in vitro and angiogenesis in vivo. Hyal1 levels are high in two human breast cancer cell lines (i.e. MDA-MB-231 and MCF-7) and in metastatic lymph nodes of breast cancer patients [4].
Hyal2 expression has been correlated with progression of multiple cancers with the availability of isozyme-specific antibodies. In some cases, loss of Hyal2 expression has been reported, e.g. in a small-scale study of human lung cancer [5] or in endometrial cancer relative to normal tissue [6]. In contrast, expression of Hyal2 was significantly increased in pre-malignant and malignant melanomas [7] and in breast cancer specimens, specifically at the expanding margins of invasive breast cancer [4, 8]. The other three human hyaluronidase family members, Hyal3, Hyal4 and PH-20, have been studied to a lesser extent in relation to cancer.
Hyaluronidase demonstrated potential for clinical utility to improve the absorption of extravasated drugs into circulation where they can be metabolised. It is used in many fields, for example to enhance the absorption of fluids given by subcutaneous or intramuscular injections or to improve the diffusion of local anesthetics. Furthermore, it is used in enhancing the actions of anticancer drugs by increasing drug penetration into the tumour; this is where hyaluronidase finds its clinical utility.
Hyaluronic acid can be found in EDTA blood samples of patients with adenocarcinoma and can lead to interferences related to the reagent system used. Sysmex’ XN-Series analysers use different measurement channels with proprietary reagents to enhance specific cell characteristics. In a CBC+DIFF measurement profile, both the WNR channel and the WDF channel are used to count and differentiate white blood cells. Both measurement channels use a completely different set of reagents, containing a lysis and fluorescence reagent. Whereas the lysis reagent in the WNR channel extensively damages the cell membranes of all white blood cells but basophils, the lysis reagent in the WDF perforates the cell membranes while leaving the cells largely intact. Therefore, differences in the WBC counts from the WNR and WDF channels can occur and are even used by the XN-Series analyser to detect interferences in the measurement channels.
Numerical results
The complete blood count results showed values within the reference range.
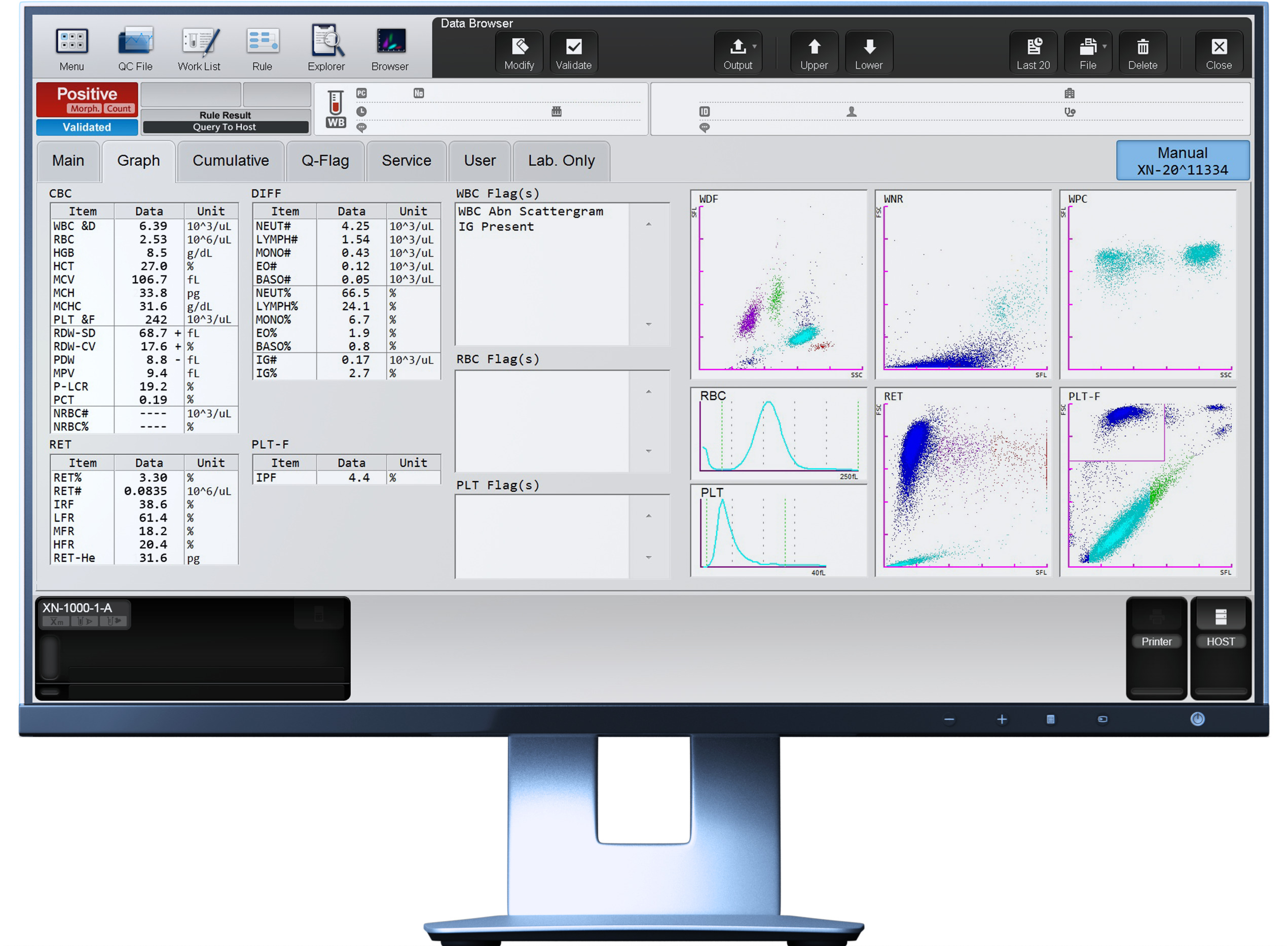
Scattergram interpretation
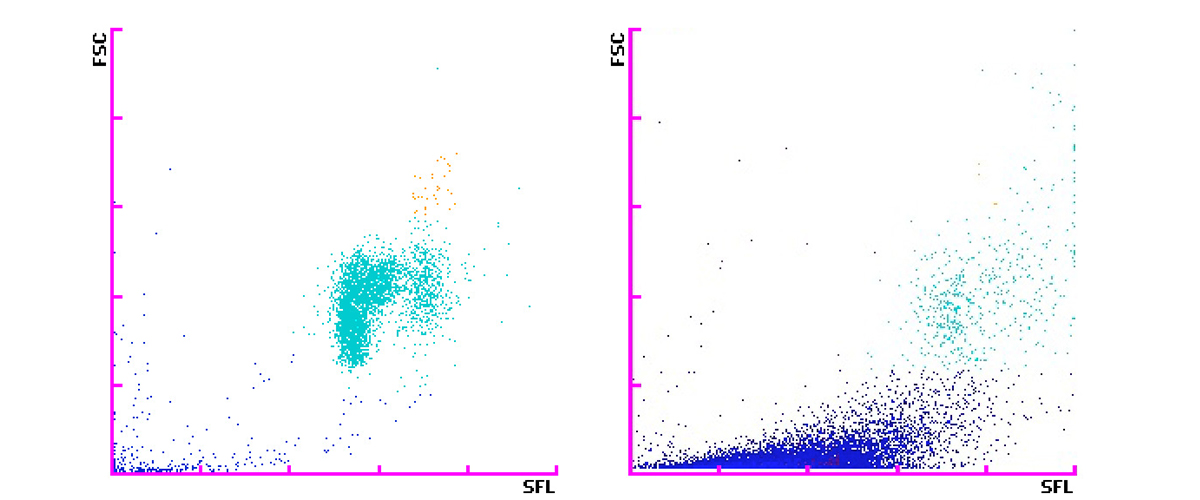
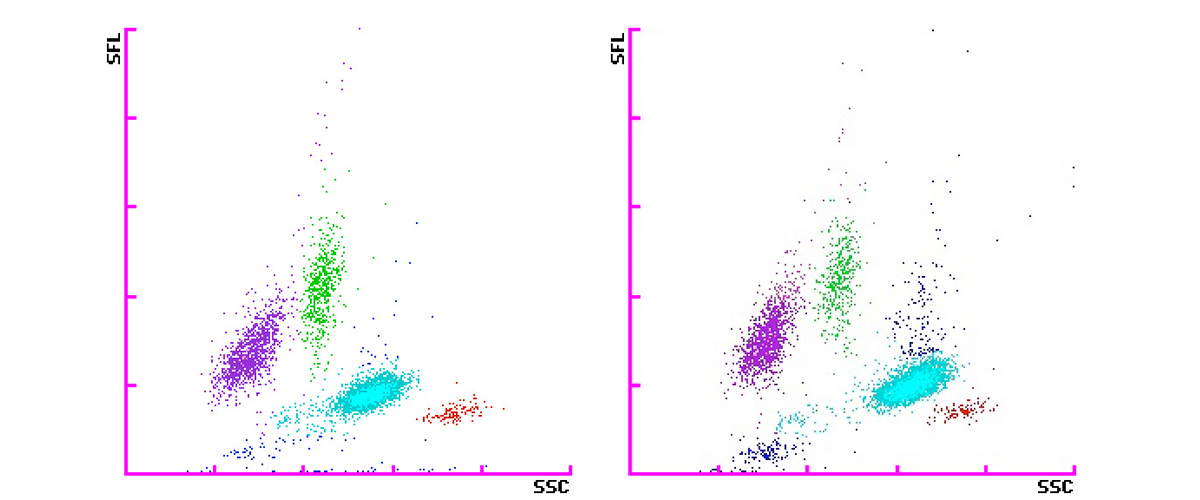
Below are WNR and WDF scattergrams determined on a XN-Series haematology analyser from a patient diagnosed with ossal and hepatogenic metastatic mammary carcinoma with progression under capecitabine treatment.
The WNR channel shows intense debris leading to the flag ʿWBC Abn Scattergramʾ whereas the WDF scattergram shows a completely normal distribution of cells. An association between an increased WBC lysis or aggregation in the acidic WNR channel and adenocarcinoma could be hypothesised.
The hypersecretion of hyaluronic acid of this patient could cause an aggregation or hyperlysis of the WBC only with the acidic WNR reagent, but not with the reagents used in the WDF channel. WBC counts generated by the WNR channel become falsely low, while those of the WDF and WPC channels are not affected by this phenomenon [9]. Therefore, the algorithms of the XN-Series analysers detect this interference and automatically report the correct WBC count obtained from the WDF channel indicated by WBC&D.
The analyser also produced the ʿIG presentʾ flag, which informs the user about an increased immature granulocyte count, in this case accounting for 2.7% of the total WBC. This results from infiltration and replacement of bone marrow cells through metastasis and is consistent with the clinical findings that metastases were still present in the bone marrow (myelophthisis), so the patient would need to be monitored continuously under treatment.
Scattergrams of WNR and WDF measurement channels
References
[1] Tan JX et al. (2011) Upregulation of HYAL1 Expression in Breast Cancer Promoted Tumor Cell Proliferation, Migration, Invasion and Angiogenesis. PLoS ONE 6(7): e22836.
[2] McAttee CO et al. (2014) Emerging roles for hyaluronidase in cancer metastasis and therapy. Adv Cancer Res. 2014 ; 123: 1–34.
[3] Poola I et al. (2008) Molecular risk assessment for breast cancer development in patients with ductal hyperplasias. Clin Cancer Res. 14:1274–80.
[4] Tan JX et al. (2011) HYAL1 overexpression is correlated with the malignant behavior of human breast cancer. Int J Cancer. 2011a;128:1303–15.
[5] Li R et al. (2007) Genetic deletions in sputum as diagnostic markers for early detection of stage I non-small cell lung cancer. Clin Cancer Res. 13:482–87.
[6] Nykopp TK et al. (2010) Hyaluronan synthases (HAS1-3) and hyaluronidases (HYAL1-2) in the accumulation of hyaluronan in endometrioid endometrial carcinoma. BMC Cancer. 2010;10:512.
[7] Siiskonen H et al. (2013) Inverse expression of hyaluronidase 2 and hyaluronan synthases 1-3 is associated with reduced hyaluronan content in malignant cutaneous melanoma. BMC Cancer. 2013;13:181.
[8] Udabage L et al. (2005) The over-expression of HAS2, Hyal-2 and CD44 is implicated in the invasiveness of breast cancer. Exp Cell Res. 2005;310:205–17.
[9] Nguyen VTP et al. (2015) Spurious decrease in the WBC count measured by the WNR channel of XN haematology analyser (Sysmex) could be associated with metastatic adenocarcinoma. Int J Lab Hematol. 37(5) e129-e132

