
Scientific Calendar August 2020
What is typically observed during an early phase of acute bacterial infection using results from a haematology analyser?
Immature granulocytes and a high Delta-He value
A high RET-He value
Neutrophil activation and a low-to-negative Delta-He value
A low MicroR value
Congratulations!
That's the correct answer!
Sorry! That´s not completely correct!
Please try again
Sorry! That's not the correct answer!
Please try again
Notice
Please select at least one answer
Scientific background
Sepsis is an organism’s systemic response to an uncontrolled spread of infection due to invading pathogens. The main characteristic of sepsis is that the body damages its own tissue and organs due to an overshooting inflammatory response to a systemic infection. If untreated, sepsis impressively quickly turns to septic shock with multiple organ failure, leading to serious life-threatening conditions and potentially death.
It is remarkable that any local infection from urinary tract infection to tonsillitis can evolve into sepsis. The pathogens and the corresponding toxins of the initially infected site manage to overcome the local immune defence mechanisms of the body and enter the circular peripheral blood.
One of the first-line defence cells of the host’s innate immune response are the neutrophils, which significantly increase in number and activation after the local infection becomes more systemic. Activated neutrophils migrate from the blood stream to the infected tissue. Upon arrival, neutrophils can effectively capture, engulf, phagocyte and kill invading microorganisms [1-3].
How do neutrophils do this? Activated and attracted by various cytokines of the CXC class (e.g. Interleukin-8), neutrophils in infected tissue form net-like structures called ‘neutrophil extracellular traps’ (NETs) [1]. This process is called ‘NETosis’. NETs are produced due to the cell’s release of its nucleic acid content, condensed as chromatin, which makes up the main component of NETs, together with other proteins. In combination with the secretion of antimicrobial components from their granule, the formation of NETs enables neutrophils to capture, phagocyte and kill bacteria and larger pathogens like fungi. Moreover, recent publications revealed the major role of NETs in linking inflammation, immunity and haemostasis [2, 3]. They seem to be condensation structures for the pathogenesis of disseminated intravascular coagulation (DIC) resulting in microthrombi nowadays – a phenomenon known as immunothrombosis [2].
Hence, in septic conditions, overstimulation of the host’s immune response and falsely signalling during pathogen recognition lead to overactivated neutrophils and therefore many vascular NETs [2, 3]. This can cause hypercoagulability during septic shock and result in severe tissue damage and organ failure.
The two haematological parameters NEUT-RI (neutrophil reactivity intensity) and NEUT-GI (neutrophil granularity intensity) of the Sysmex XN-Series indicate the neutrophil cell activation and can support early infection recognition [3-5, 10].
Numerical results
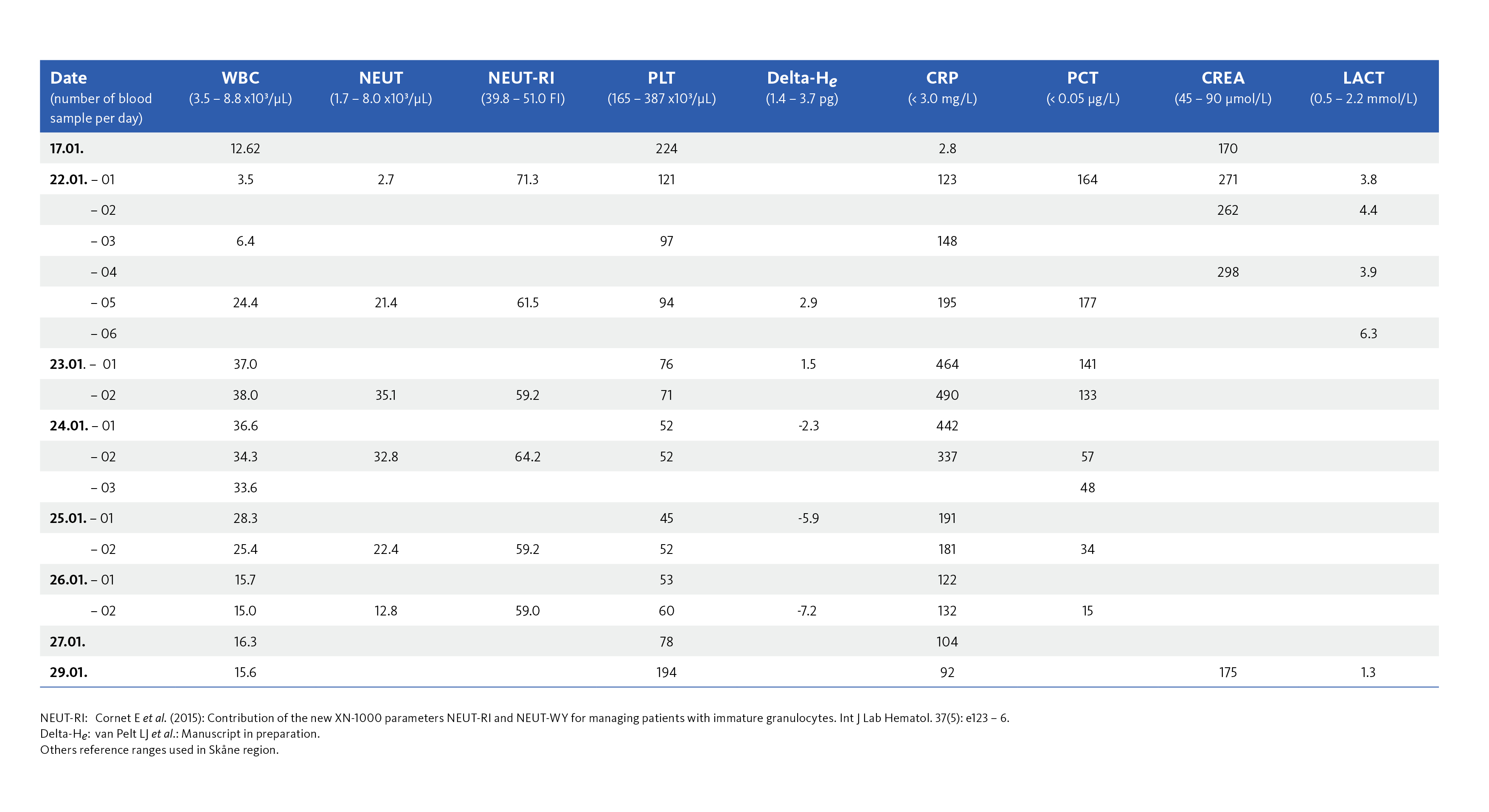
The first XN results of the 67-year old woman after she was diagnosed with pyelonephritis revealed a slightly decreased WBC count (3.5 x10³/µL) in the morning. While closely monitoring her during the day, it was seen in the afternoon that the WBC count increased to a level of 24.4 x10³/µL with highly elevated neutrophil count (21.2 x10³/µL) (without immature granulocytes) and mild thrombocytopenia. Classical biochemistry inflammation markers were strongly elevated, CRP = 195 mg/dL and PCT = 177 µg/L.
To assess the innate immune response to pathogens, several indicative parameters from the XN results could be considered as the aid in the diagnosis.
NEUT-RI
In the WDF channel, the neutrophils showed very high activation – NEUT-RI = 71.3 FI (FI = fluorescence intensity; the reference range is 39.8 – 51.0 FI [4]) whereas lymphocyte activation parameters including reactive lymphocytes (RE-LYMP) and antibody-synthesizing lymphocytes (AS-LYMP) did not show any sign of activation. This could typically indicate the early innate immune response against bacterial pathogens [5].
Delta-He
Delta-He is the difference between the haemoglobin content of reticulocytes (RET-He) and the haemoglobin content of the mature red blood cells (RBC-He). Under normal physiological conditions Delta-He is a positive value between + 1.4 pg and + 3.7 pg [6] but turns negative within a few hours because there is an iron deficiency due to inflammation [7]. Iron sequestration by ferritin in macrophages restricts iron availability for extracellularly occurring pathogens. The mechanism suppresses iron availability to the erythropoietic progenitor cells by retaining iron in the macrophages. If the Delta-He value suddenly drops to negative value, there is the suspicion that the patient most likely has an acute phase reaction or might develop severe infection course [8]. Danielson et al. observed a correlation of Delta-He with the biochemistry markers IL-6 and hs-CRP [9].
During the first measurement of the patient’s blood sample, a normal Delta-He value (Delta-He = 2.9 pg) was observed. However, results over the next few days showed a strong decreasing trend and the Delta-He value turned negative.
The diagnosis of bacterial sepsis was confirmed by a blood culture positive for Escherichia coli derived from the previous pyelonephritis. Antibiotic treatment was started immediately together with the administration of intravenous fluid and other medical interventions.
Platelets and IPF
The platelet results showed mild thrombocytopenia at the time of measurement when the sepsis was suspected and decreased even further during the time course. Development of thrombocytopenia during sepsis is complex, involves several factors and is associated with a poor prognosis in critically ill patients. For example, endothelial dysfunction is one major consequence of sepsis and plays a critical role in platelet activation and consumption.
Immature platelet fraction (IPF) is a platelet parameter which reflects the ratio of young, immature platelets in the total platelet count. Studies performed in the last years suggest that IPF can provide clinically relevant information about inflammatory activity and disease prognosis [10-12]. In the context of sepsis, a recent study conducted in critically ill patients suggested that the IPF increases before sepsis becomes clinically manifested and may provide valuable clinical information for predicting the risk of developing clinically evident systemic infections [13].
The table shows selected haematological and biochemistry parameters of the patient during the stay at the intensive care unit.
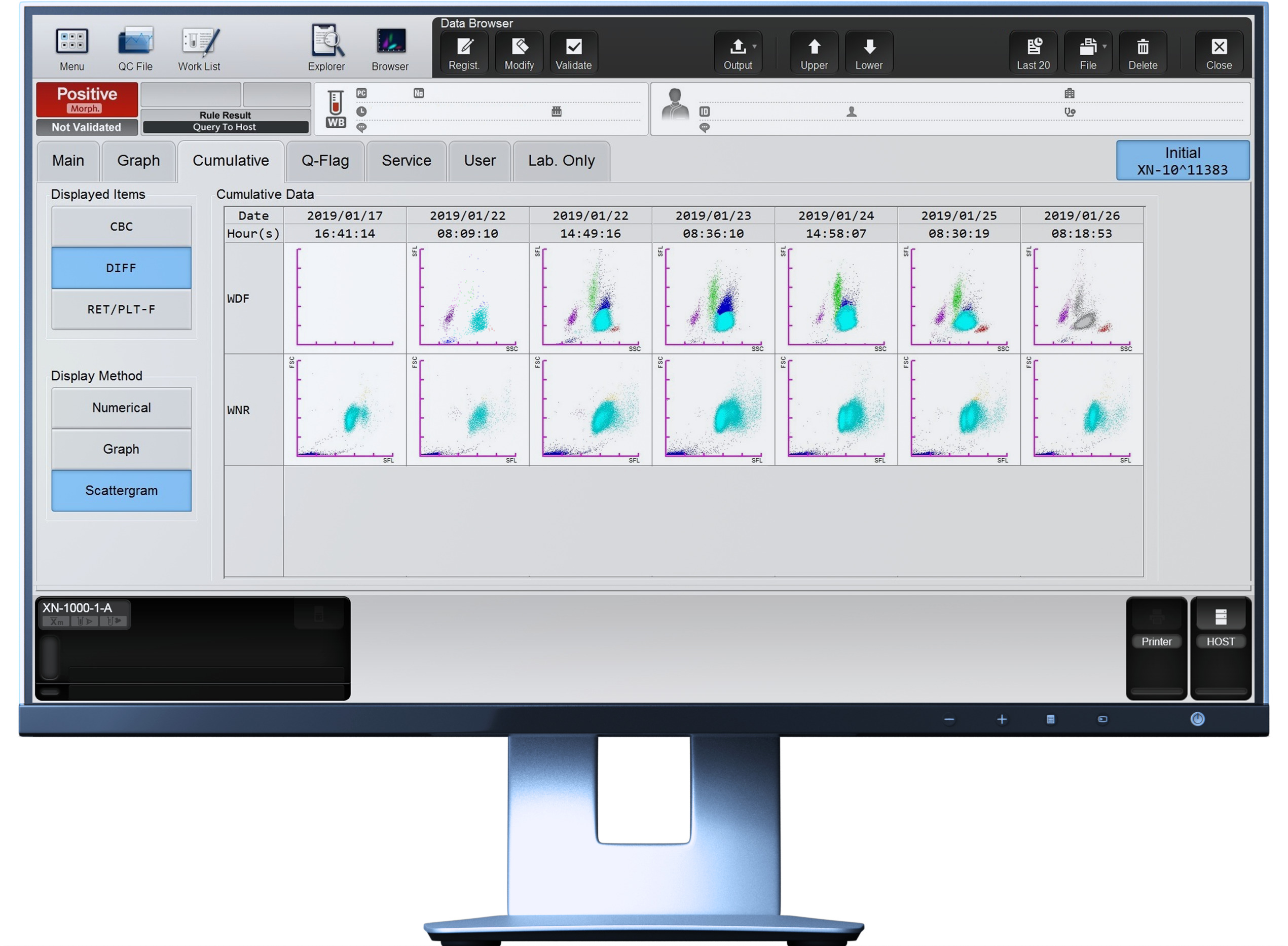
Scattergram interpretation
The interesting part of this view is the dynamics of the neutrophil cloud (light blue) over the period of time. Neutrophils are one of the first cells of the innate immune response to counter bacterial infections. The morphological change in granulation and metabolic activity of activated neutrophils is reflected by the XN parameters NEUT-GI and NEUT-RI. This can also be seen in the shape of the neutrophil cloud (e.g. elongation of the cloud because of increasing fluorescence activity). Systemic inflammation increases the de novo production of neutrophils and enhances the mobilisation of immature neutrophils into circulation, a phenomenon known as ‘emergency granulopoiesis’ [14]. This can also be seen in this patient case looking at the rapid increase of neutrophils and subsequent increase of immature granulocytes (dark blue) in the scattergrams.
This case was shared by our customers from Klinisk kemi (Clinical Chemistry department) in the region of Skåne, Sweden. We sincerely thank our customers for the contribution to our scientific calendar.
References
[1] Brinkmann V et al. (2004): Neutrophil extracellular traps kill bacteria. Science. 303(5663):1532‐1535.
[2] Delabranche X et al. (2017): Evidence of Netosis in Septic Shock-Induced Disseminated Intravascular Coagulation. SHOCK. 47(3):313-317.
[3] Stiel L et al. (2016): Neutrophil Fluorescence: A New Indicator of Cell Activation During Septic Shock-Induced Disseminated Intravascular Coagulation. Crit Care Med. 44(11): e1132–36.
[4] Cornet E et al. (2015): Contribution of the new XN-1000 parameters NEUT-RI and NEUT-WY for managing patients with immature granulocytes. Int J Lab Hematol. 37(5): e123-6.
[5] Ustyantseva M et al. (2019): Innovative Technologies in the Evaluation of the Neutrophil Functional Activity in Sepsis. Sysmex Journal International. 29(1): 8.
Sysmex Journal International: https://www.sysmex.co.jp/en/products_solutions/library/journal/index.html
[6] van Pelt LJ et al.: Manuscript in preparation.
[7] Interview with Adjunct Professor Dr Mathias Zimmermann, specialist in laboratory medicine and Head Physician of the Central Department for Laboratory Medicine at the DRK (German Red Cross) hospitals in Berlin. Accessed on 18.06.2020 https://www.sysmex-europe.com/n/academy/knowledge-centre/expert-interviews/haematology/tracing-iron-deficiency-part-1.html
[8] Weimann A et al. (2016): Delta-He, Ret-He and a New Diagnostic Plot for Differential Diagnosis and Therapy Monitoring of Patients Suffering from Various Disease-Specific Types of Anemia. Clin Lab. 62(4): 667.
[9] Danielson K et al. (2014): Delta-He: A novel marker of inflammation predicting mortality and ESA response in peritoneal dialysis patients. Clin Kidney J. 7(3): 275-281.
[10] Hong KH et al. (2009): Prognostic Value of Immature Platelet Fraction and Plasma Thrombo-poietin in Disseminated Intravascular Coagulation. Blood Coagul Fibrinolysis. Sep;20(6):409-14.
[11] Hubert RME et al. (2015): Association of the immature platelet fraction with sepsis diagnosis and severity. Sci Rep. 5: 8019.
[12] Muronoi T et al. (2016): Immature platelet fraction predicts coagulopathy-related platelet consumption and mortality in patients with sepsis. Thromb Res. 144: 169-75.
[13] Buoro S et al. (2018): Innovative haematological parameters for early diagnosis of sepsis in adult patients admitted in intensive care unit. J Clin Pathol. 71(4): 330.
[14] Hong CW (2017): Current Understanding in Neutrophil Differentiation and Heterogeneity. Immune Netw. 17(5):298-306.


