
Chronic kidney disease diagnostics and surveillance
Chronic kidney disease (CKD) can be defined as persistent abnormalities of the kidney structure and function that are present for a minimum of three months.
With diabetes and hypertension contributing to around two thirds of all CKD cases, the global prevalence of CKD of 9.1% in 2017 positively correlates with the increasing prevalence of those diseases.
The global burden of CKD
Chronic kidney disease diminishes patients’ quality of life, especially at a later stage when CKD progresses into end-stage renal failure and renal replacement therapies (RRT) become necessary. High healthcare expenditures and socio-economic disadvantages are additional consequences.
- 5.4 million people will require RRT (renal replacement therapy) by 2030.
- 36 million disability-adjusted life-years (DALYs) are accumulated among CKD patients.
- Estimated annual costs are 45000€ per stage five CKD patient.
This healthcare burden will further increase; by 2040, CKD is expected to become the fifth most common cause of death.
Prevention
Since the development of CKD can be reverted or its progression slowed down if detected at an early stage, a regular screening of risk patients for the disease’s onset can help ease the burden and fight CKD.
Albuminuria
Albuminuria, the presence of albumin in urine, is a key indicator for glomerular damage and the onset and progression of kidney disease; it is also a marker of premature death.
Albuminuria is often already present when eGFR is still normal and thus can indicate kidney damage at an earlier stage.
Can a test strip support the fight against the burden of CKD?
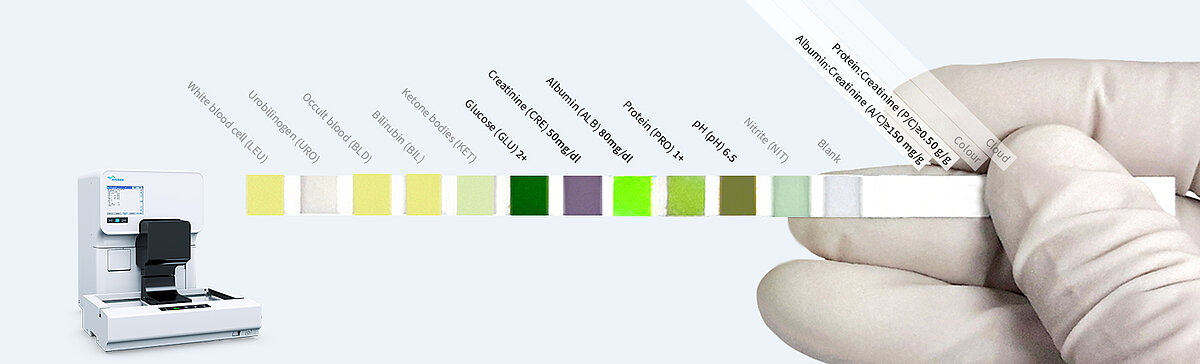
The Sysmex Meditape 11A test strips are classic dye-binding-based dry chemistry sticks that detect and quantify various urinary parameters, including albumin and creatinine, to accurately measure the albumin to creatinine ratio (ACR) by accounting for the physiological variation of urinary albumin levels.
In combination with a reflectance measurement using the CMOS technology of the UC-3500, the Meditape 11A test strip allows the sensitive and accurate detection of albuminuria at physiological levels. With a limit of detection as low as 5.5 mg/L and a reportable range of 10 mg/L, the Meditape 11A test strip in combination with the UC-3500 reaches measurement ranges that compare to traditional immunonephelometric assays, allowing the quantification of albuminuria at an early stage.
Considering the comparatively low costs for test strip-based techniques, economic considerations might no longer prevent a broad screening approach for CKD among risk group patients.
Fostering early detection of the onset of CKD in risk group patients
At the University Hospital San Juan (Alicante, Spain), Dr María Salínas, Head of Clinical Analytical Services, and her team investigated the potential of the automated test strip analysis on the UC-3500 to replace quantitative tests. Here, a new workflow was concluded, with test strip analysis as the default screening for albuminuria. Upon exceeding defined cut-off values (≥ 10 mg/L albumin and ≥ 4.42 mmol/L creatinine), samples are flagged for a suspected increased albumin:creatinine ratio (ACR) and are subjected to quantitative assessment [6].
Meanwhile, the laboratory was able to reduce the need for quantitative assessments of albuminuria by up to 80%, resulting in remarkable cost savings. These savings are directly converted into additional capacities for screening risk group individuals for the disease’s onset. This allows a wider-ranging early detection of CKD, supporting efforts to reduce the healthcare burden it represents (Fig. 5).
However, the laboratory at the University Hospital San Juan has capitalised on these advantages beyond the immediate scope of CKD, using the cost savings to screen for other occult diseases, such as diabetes. The early detection of these diseases allows early treatment to revert or at least slow down disease progression, with a positive impact on public health and social costs [Publication in preparation].
Here, screening is performed using defined algorithms that consider patient history, public health data and clinical practice guidelines, lifting laboratory diagnostics to the next level – not only by highlighting the importance of laboratory diagnostics but also by strengthening the role of the clinical laboratory as a hub for decision-making [9].
Deeper insight into the kidney status
For extended diagnostics beyond the detection of albuminuria, the UN-Series can provide deeper insights into kidney abnormalities by detecting related urinary abnormalities and informing about their glomerular or tubular origin.
Haematuria
Haematuria is detected and quantified, even at low levels, by the UF-series using fluorescence flow cytometry. The related scattergram pattern allows the differentiation of isomorphic and dysmorphic red blood cells and in turn supports the determination of the cause of haematuria, since dysmorphic RBCs are an indicator of a glomerular origin of haematuria.
Casts
- Casts are detected, quantified and differentiated into hyaline and pathological casts by the UF-series
- Hyaline casts (Hy.Cast) are commonly detected in kidney disorders but also have non-renal causes, such as exercise, fever or dehydration
- Pathological casts (Path.Cast) are a sensitive diagnostic indicator of substantial kidney damage (eg erythrocyte casts in glomerulonephritis)

RTEC
Renal tubular epithelial cells (RTECs) are commonly observed in urine samples in the case of kidney injuries, upper urinary tract infections and glomerular and tubular damage. The UF-series detects and quantifies RTEC, supporting the detection of renal damage.
References
[1] Decavele AS, Fiers T, Penders J and Delanghe JR (2012): A sensitive quantitative test strip based albuminuria screening assay. Clin Chem Lab Med 50(4):673-678
[2] Delanghe JR, Himpe J, De Cock N, Delanghe S, De Herde K, Stove V and Speeckaert MM (2017): Sensitive albuminuria analysis using dye-binding based test strip. Clin Chim Acta 471:107-112
[3] Enko D, Stelzer I, Boeckl M, Derler BSchnedl WJ, Anderssohn P, Meinitzer A and Herrmann M (2020): Comparison of the diagnostic performance of two automated urine sediment analyzers with manual phase-contrast microscopy. Clin Chem Lab Med 58(2):268-273
[4] Fairley KF, Birch DF (1982): Haematuria: a simple method for identifying glomerular bleeding. Kidney Int 21:105-108.
[5] Forouzanfar MH et al. (2017): Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115mmHg, 1990-2015. JAMA 317(2):165-182
[6] GBD Chronic Kidney Disease Collaboration (2020): Global, regional, and national burden of chronic kidney disease 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 395(10225):709-733
[7] KDIGO (2012): Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3: 1–150
[8] Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H and Al Kaabi J (2020): Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted Trends. Journal of Epidemiology and Global Health 10(1):107–111
[9] Oyaert M and Delanghe JR (2019): Semiquantitative, Fully Automated Urine Test Strip Analysis. J Clin Lab Anal 33(5):e22870
[10] Oyaert M, Speeckaert M, Boelens J and Delanghe JR (2020): Renal Tubular Epithelial Cells Add Value in the Diagnosis of Upper Urinary Tract Pathology. Clin Chem Lab Med 58(4):597-604
[11] Salínas M, López-Garrigós M, Flores E, Lugo J, Leiva-Salínas C and PRIMary Care-LABoratory (PRIMLAB) working group (2018): Urinary albumin strip assay as a screening test to replace quantitative technology in certain conditions. Clin Chem Lab Med 57(2):204-209
LAB – References
[1] Delanghe JR, Himpe J, De Cock N, Delanghe S, De Herde K, Stove V and Speeckaert MM (2018): Urinary albumin strip assay as a screening test to replace quantitative technology in certain conditions. Clin Chem Lab Med. 19;57(2):204-209.
[2] GBD Chronic Kidney Disease Collaboration (2020): Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet
[3] Forouzanfar MH et al. (2017): Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115mmHg, 1990-2015. JAMA 317(2):165-182
[4] KDIGO (2012): Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3: 1–150
[5] Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H and Al Kaabi J (2020): Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted Trends. Journal of Epidemiology and Global Health 10(1):107–111
[6] Salínas M, López-Garrigós M, Flores E, Lugo J, Leiva-Salínas C and PRIMary Care-LABoratory (PRIMLAB) working group (2018): Urinary albumin strip assay as a screening test to replace quantitative technology in certain conditions. Clin Chem Lab Med 57(2):204-209






